


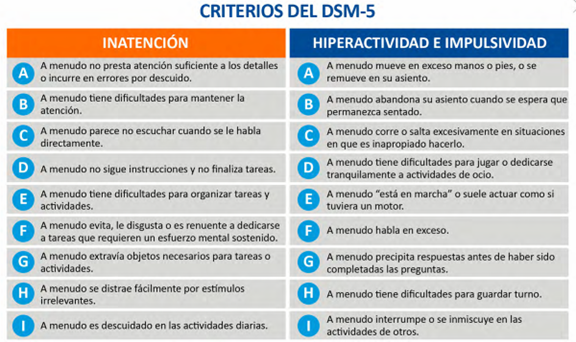
Criterios del DSM-5 para Diagnóstico de TDAH
Es necesario que al menos seis de los siguientes síntomas hayan persistido durante un mínimo de seis meses:
Referencias
1. American Psychiatric Association (2014). Manual Diagnóstico y Estadístico de los Transtornos Mentales (DSM-5), 5ª Ed. Madrid: Editorial Médica Panamericana.
Inicio
![]() Nota
Nota
RELEVANCIA DEL DIAGNÓSTICO PRECISO DEL TIPO DE CRISIS EN LOS PACIENTES CON TRASTORNOS EPILÉPTICOS
La precisión diagnóstica del tipo de crisis tiene creciente relevancia en el manejo contemporáneo de los pacientes con trastornos epilépticos.1-6
De hecho, es un componente esencial del enfoque de medicina de precisión, el cual reconoce la importancia de un abordaje individualizado en lugar de una aproximación terapéutica uniforme, para la elección del tratamiento.1,2,4,7-9
El diagnóstico preciso del tipo de crisis es fundamental para:1-3,5,6,9-13
- La clasificación correcta del síndrome epiléptico.
- La implementación de intervenciones médicas exitosas.
- La toma de decisiones terapéuticas.
- La selección del agente antiepiléptico.
La clasificación vigente de la ILAE (International League Against Epilepsy) enfatiza la semiología (fenomenología) de la crisis, la etiología de la misma y la categorización sindromática.1,3,10-12,14,15
El análisis fenomenológico del tipo de crisis implica una documentación objetiva e integral de la crisis, para la diferenciación entre los distintos tipos.1,5,14,16
Referencias
1. Abdelsamad A, Kachhadia MP, Hassan T, et al. Charting the progress of epilepsy classification: navigating a shifting landscape. Cureus 2023; 15: e46470.
2. Boon P, Ferrao Santos S, Jansen AC, et al. Recommendations for the treatment of epilepsy in adult and pediatric patientes in Belgium: 2020 update. Acta Neurol Belg 2021; 121: 241-57.
3. HakamiT. Efficacy and tolerability of antiseizure drugs. Ther Adv Neurol Disord 2021; 14: 1-21.
4. Gunasekera CL, Sirven JI, Feyissa AM. The evolution of antiseizure medication therapy selecion in adults: is artificial intelligen ce-assisted antiseizure medication selection ready for prime time? J Centr nerv Syst Dis 2023; 15: 11795735231209209.
5. Grönheit W, Behrens V, Liakina T, et al. Teaching distinguishing semiological features improves diagnostic accuracy of seizure-like events by emergency physicians. Neurol Res Pract 2022; 4: 56-64.
6. Lado FA, Ahrens SM, riker E, et al. Guidelines for specialized epilepsy centers: Executive summary of the Report of the National Association of Epilepsy Centers guideline panel. Neurology 2024; 102: e208087.
7. Chaplin S. Update guideline on diagnosing and managing epilepsies. Prescriber 2022; 33: 28-30.
8. Ghosh S, Sinha JK, Ghosh S, et al. A comprehensive review of emerging trends and innovative therapies in epilepsy management. Brain Sci 2023; 13: 1305-31.
9. National Institute for Health and Care Excellence (NICE). Epilepsies in children, young people and adults. 2022 Apr 27: 35700280.
10. Wirrell E, Tinuper P, Perucca E, Moshé SL. Introduction to the epilepsy syndrome papers. Epilepsia 2022; 63: 1330-2.
11. Perucca P, Scheffer IE, Kiley M. The management of epilepsy in children and adults. Med J Aust 2018; 208: 226-33.
12. D’Onofrio G, roberti R, Riva A, et al. Pharmacodynamic rationale for the choice of antiseizure medications in the paediatric popula tion. Neurotherapeutics 2024; 21: e00344.
13. Löscher W, Klein P. The pharmacology and clinical efficacy of antiseizure medications: from bromide salts to cenobamate and beyond.CNS Drugs 2021; 35: 935-63.
14. Beniczky S, Tatum WO, Blumenfeld H, et al. Seizure semiology: ILAE glossary of terms and their significance. Epileptic Disord 2022; 24: 447-95.
15. Scheffer IE, Berkovic S, Capovilla G, et al. ILAE classification of the epilepsies position paper of the ILAE Commission for Classifica tion and Terminology. Epilepsia 2017; 58: 512-21.
16. Wolf P, Benbadis S, Dimova PS, et al. The importance of semiological information based on epileptic seizure history. Epileptic Disord 2020; 22: 15-31.
Inicio
![]() Nota
Nota
¿CUÁLES SON LOS ESCENARIOS CLÍNICOS EN DONDE DIVALPROATO ES PARTICULARMENTE ÚTIL?

Entre los aspectos a considerar al momento de seleccionar la terapia farmacológica, en los pacientes con trastornos epilépticos, es fundamental tener en cuenta que ciertos fármacos pueden exacerbar determinados tipos de crisis.1-8
Los agentes anticrisis de espectro reducido están asociados a una mayor probabilidad de exacerbación paradójica de las crisis, que los de amplio espectro.3,6,9
En los pacientes con crisis de ausencias o crisis mioclónicas (incluyendo la epilepsia mioclónica juvenil), los siguientes agentes pueden exacerbar las crisis: carbamazepina, lamotrigina, gabapentín, oxcarbazepina, fenitoína, pregabalina, tiagabina y vigabatrín.2-7,10
Carbamazepina, gabapentín, oxcarbazepina, pregabalina, tiagabina y vigabatrín pueden inducir exacerbación paradójica en los pacientes con crisis tónicas o atónicas.2,5
En los pacientes con crisis generalizadas tónico-clónicas la exacerbación paradójica está asociada principalmente al uso de agentes de espectro reducido (efectivos contra crisis focales), tales como:3,4,6,7-11
- Carbamazepina.
- Gabapentín.
- Oxcarbazepina.
- Fenitoína.
- Tiagabina.
- Vigabatrín.
En el grupo de epilepsias idiopáticas generalizadas, así como en el grupo de epilepsias de causa desconocida, el valproato es mejor tolerado. 12, 13
Referencias
1. Chaplin S. Update guideline on diagnosing and managing epilepsies. Prescriber 2022; 33: 28-30.
2. National Institute for Health and Excellence (NiCE). Epilepsies in children, young people and adults. NICE, 2022; PMID: 35700280.
3. D’Onofrio G, roberti R, Riva A, et al. Pharmacodynamic rationale for the choice of antiseizure medications in the paediatric population. Neurotherapeutics 2024; 21: e00344.
4. Gunasekera CL, Sirven JI, Feyissa AM. The evolution of antiseizure medication therapy selecion in adults: is artificial intelligence-assisted antiseizure medication selection ready for prime time? J Centr nerv Syst Dis 2023; 15: 11795735231209209.
5. Boon P, Ferrao Santos S, Jansen AC, et al. Recommendations for the treatment of epilepsy in adult and pediatric patientes in Belgium: 2020 update. Acta Neurol Belg 2021; 121: 241-57.
6. Hirsch E, French J, Scheffer IE, et al. ILAE definition of the idiopathic generalized epilepsy syndromes: position statement by the ILAE Task Force on Nosology and Definitions. Epilepsia 2022; 63: 1475-99.
7. Hakami T. Neuropharmacology of antiseizure drugs. Neuropsychopharmacol Rep 2021; 41: 336-51.
8. Löscher W, Klein P. The pharmacology and clinical efficacy of antiseizure medications: from bromide salts to cenobamate and beyond.CNS Drugs 2021; 35: 935-63.
9. Jaramillo MA, Pham T, Kamrudin S, et al. Seizure exacerbation with anti-seizure medications in adult patients with epilepsy. Epilepsy Res 2022; 181: 106885.
10. HakamiT. Efficacy and tolerability of antiseizure drugs. Ther Adv Neurol Disord 2021; 14: 1-21.
11. Wolf P, Benbadis S, Dimova PS, et al. The importance of semiological information based on epileptic seizure history. 2020; 22: 15-31.
12. Marson AG, Al-Kharusi AM, Alwaidh M, et al. The SANAD study of effectiveness of valproate, lamotrigine, or topiramate for generalised and unclassifiable epilepsy: an unblinded randomised controlled trial. Lancet. 2007.
13. Marson A, Burnside G, Appleton R, et al The SANAD II study of the effectiveness and cost-effectiveness of valproate versus levetiracetam for newly diagnosed generalized and unclassifiable epilepsy: an open-label, non-inferiority, multicentre, phase 4, randomised controlled trial. Lancet. 2021
Inicio
![]() Nota
Nota
¿Qué relación existe entre el insomnio y la depresión?

Los pacientes con trastornos depresivos exhiben una secreción disminuida de melatonina y los nive les nocturnos de esta tienen una correlación inversa con la severidad de la depresión.1,7
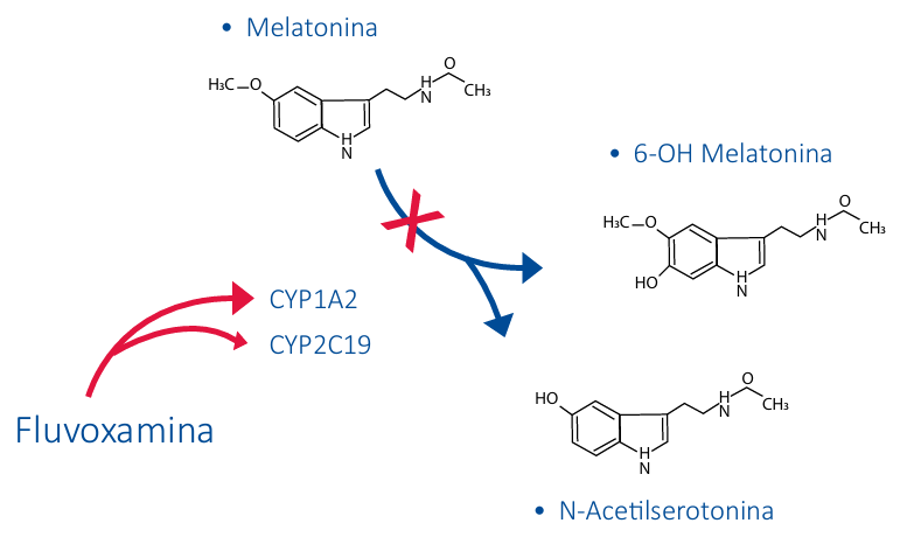
La terapia con fluvoxamina está asociada a un incremento significativo de las concentraciones plasmáticas de melatonina, durante la noche y en las primeras horas del día.1,2,8,11
Ello se debe, principalmente, a que el metabolismo hepático de fluvoxamina induce la inhibición de las enzimas CYP1A2 y CYP2C19, responsables de la degradación de la melatonina.2,9,12
Referencias
1. Silva S, Bicker J, Falcao A, Fortuna A. Antidepressants and circadian rhythm: exploring their bidirectional interaction for the treatment of depression. Pharmaceutics 2021; 13: 1975-2008.
2. Sunami E, Usuda K, Nishiyama Y, et al. A preliminary study of fluvoxamine maleate on depressive state and serum melatonin levels in patients after cerebral infarction. Intern Med 2012; 51: 1187-93.
3. Charrier A, Olliac B, Roubertoux P, Tordjman S. Clock genes and altered sleep-wake rhythms: their role in the development of psychiatric disorders. Int J Mol Sci 2017; 18: 938-59. 4. Boiko DI, Shkodina AD, Hasan MM, et al. Melatonergic receptors (Mt1/Mt2) as a potential additional target on novel drugs for depression. Neurochem Res 2022; 47: 2909-24.
5. Lesicka M, Dmitrazk-Weglarz M, Jablonska E, et al. Methylation of melatonin receptors in patients with unipolar and bipolar depression. mech Ageing Dev 2023; 211: 111776.
6. Wang YQ, Jiang YJ, Zou MS, et al. Antidepressant actions of melatonin and melatonin receptor agonist: focus on pathophysiology and treatment. Behav Brain Res 2022; 420: 113724.
7. Li C, Ma D, Li M, et al. The therapeutic effect of exogenous melatonin on depressive symptoms: a systematic review and meta-analysis. Front Psychiatry 2022; 13: 737972.
8. Wilde MI, Plosker GL, Benfield P. Fluvoxamine: an update review of its pharmacology, and therapeutic use in depressive illness. Drugs 1993; 46: 895-924.
9. Von Bahar C, Ursing C, Yasui N, et al. Fluvoxamine but not citalopram increases serum melatonin in healthy subjects – an indication that cytochrome P450 CYP1A2 and CYP2C19 hydroxylate melatonin. Eur J Clin Pharmacol 2000; 56: 123-7.
10. Härtter S, Wang X, Weigmann H, et al. Differential effects of fluvoxamine and other antidepressants on the biotransformation of melatonin. J Clin Psychopharmacol 2001; 21: 167-74.
11. Hao Y, Hu Y, Wang H, et al. The effect of fluvoxamine on sleep architecture of depressed patients with insomnia: an 8-week, open-label, baseline-controlled study. Nat Sci Sleep 2019;11: 291-300.
12. Westenberg HGM, Sandner C. Tolerability and safety of fluvoxamine and other antidepressants. Int J Clin Pract 2006; 60: 482-91
Inicio
![]() Nota
Nota
Prevención de la Migraña con Divalproato
La migraña es una condición neurológica común que puede ser debilitante para quienes la padecen. El divalproato, un medicamento antiepiléptico, se ha utilizado con éxito en la prevención de la migraña. A continuación, se presenta una revisión de su eficacia y consideraciones clínicas.
Mecanismo de Acción
El divalproato actúa aumentando los niveles de ácido gamma-aminobutírico (GABA) en el cerebro, un neurotransmisor inhibidor que ayuda a estabilizar la actividad neuronal1. Este mecanismo es crucial para su efecto preventivo en la migraña, ya que reduce la hiperexcitabilidad neuronal que puede desencadenar los ataques.
Eficacia en la Prevención de la Migraña
Diversos estudios han demostrado que el divalproato es efectivo para reducir la frecuencia de los ataques de migraña. En una revisión de la Colaboración Cochrane, se encontró que el valproato (incluyendo el divalproato) redujo la frecuencia de las migrañas en aproximadamente cuatro episodios por mes en comparación con el placebo1. Además, los pacientes tratados con divalproato tenían más del doble de probabilidades de reducir el número de migrañas en un 50% o más1.
Consideraciones Clínicas
El divalproato es generalmente bien tolerado, aunque puede causar efectos secundarios como náuseas, aumento de peso y temblores. Es importante tener precaución en mujeres en edad fértil debido al riesgo de defectos de nacimiento1. La dosificación debe ser individualizada y ajustada según la respuesta del paciente y la tolerancia al medicamento2.
Comparación con Otros Tratamientos
El divalproato se compara favorablemente con otros tratamientos preventivos para la migraña, como los betabloqueadores y los antagonistas del calcio. Sin embargo, la elección del tratamiento debe ser personalizada, considerando las características individuales del paciente y la comorbilidad2.
Referencias
1. Linde M, Mulleners WM, Chronicle EP, McCrory DC. Valproate (valproic acid or sodium valproate or a combination of the two) for the prophylaxis of episodic migraine in adults. [Internet]. 2013;6. Disponible en: https://www.cochrane.org/es/CD010611/SYMPT_valproato-para-la-prevencion-de-los-ataques-de-migrana-en-adultos
2. Aguilar-Shea AL, Casanova-Peña I, Porta-Etessam J. Tratamiento preventivo de la migraña. Semergen [Internet]. 2008;34(7):336–40. Disponible en: http://dx.doi.org/10.1016/s1138-3593(08)72336-0
Inicio
![]() Nota
Nota
Dominios cognitivos afectados en pacientes con depresión mayor
El compromiso de la función cognitiva es un componente central del trastorno depresivo mayor (TDM) y está asociado a:1-9
• Deterioro funcional significativo.
• Reducción importante del éxito del tratamiento psicoterapéutico.
• Disminución sustancial de la calidad de vida.
• Incremento del suicidio.
Hasta 70%-90% de los pacientes con trastorno depresivo mayor presentan deficien cias cognitivas.1,5
De todos los inhibidores selectivos de la recaptacion de la serotonina (ISRS) Fluvoxamina es Potente agonista de receptor sigma 1 lo que permite la mejoría de la función cognitiva.3,9,11-14
Referencias
- Hammar A, Ronold EH, Rekkedal GA. Cognitive impairment and neurocognitive profiles in major depression – a clinical perspective. Front Psychiatry 2022; 13: 764374.
- Zuckerman H, Pan Z, Park C, et al. Recognition and treatment of cognitive dysfunction in major depressive disorder. Front Psychiatry 2018; 9: 655-65.
- Bobrov A, Krasnoslobodtseva L, Mutnykh E. Effects of fluvoxamine on cognitive function in outpatients with depression in remission: results of an open-label pilot study. J Psychiatry 2017; 20: 5-10.
- Niitsu T, Iyo M, Hashimoto K. Sigma-1 receptor agonists as therapeutic drugs for cognitive impairment in neuropsychiatric diseases. Curr Pharm Des 2012; 18: 875-83.
- Liu J, Dong Q, Lu X, et al. Exploration of major cognitive deficits in medication-free patients with major depressive disorder. Front Psychiatry 2019; 10: 836-43.
- Kriesche D, Woll CFJ, Tschentscher N, et al. Neurocognitive deficits in depression: a systematic review of cognitive impairment in the acute and remitted state. Eur Arch Psychiatry Clin Neurosci 2023; 273: 1105-28.
- Culpepper L, Lam RW, McIntyre RS. Cognitive impairment in patients with depression: awareness, assessment, and management. J Clin Psychiatry 2017; 78: 1383-94.
- Woo YS, Rosenblat JD, Kakar R, et al. Cognitive deficits as a mediator of poor occupational function in remitted major depressive disorder patients. Clin Psychopharmacol Neurosci 2016; 14: 1-16.
- Knight MJ, Lyrtzis E, Baune BT. The association of cognitive deficits with mental and physical quality of life in major depressive disorder. Compr Psychiatry 2020; 97: 152147.
- Ishikawa M, Ishiwata K, Ishii K, et al. High occupancy of sigma-1 receptors in the human brain after single oral administration of fluvoxamine: a positron emission tomography study using [11C]SA4503. Biol Psychiatry 2007; 62: 878-83.
- Hashimoto K. Sigma-1 receptors and selective serotonin reuptake inhibitors: clinical implications of their relationship. Cent Nerv Syst Agents Med Chem 2009; 9:197-204.
- Albayrak Y, Hashimoto K. Sigma-1 receptor agonists and their clinical implications in neuropsychiatric disorders. Adv Exp Med Biol 2017; 964: 153-61.
- Nishimura T, Ishima T, Iyo M, Hashimoto K. Potentiation of nerve growth factor-induced neurite outgrowth by fluvoxamine: role of sigma-1 receptors, IP3 receptors and cellular signaling pathways. PLoS One 2008; 3: e2558.
- Härtter S, Wang X, Weigmann H, et al. Differential effects of fluvoxamine and other antidepressants on the biotransformation of melatonin. J Clin Psychopharmacol 2001; 21: 167-74.
- Von Bahar C, Ursing C, Yasui N, et al. Fluvoxamine but not citalopram increases serum melatonin in healthy subjects – an indication that cytochrome P450 CYP1A2 and CYP2C19 hydroxylate melatonin. Eur J Clin Pharmacol 2000; 56: 123-7.
- Sunami E, Usuda K, Nishiyama Y, et al. A preliminary study of fluvoxamine maleate on depressive state and serum melatonin levels in patients after cerebral infarction. Intern Med 2012; 51: 1187-93
Inicio
![]() Nota
Nota
Abuso de alcohol y depresión
Personas con abuso de alcohol, tienen 2.3 veces más probabilidades de tener trastorno depresivo mayor.1 La prevalencia de desórdenes depresivos es mayor 3.7 veces en personas que tienen esta dependencia.1 La coexistencia de estos desordenes está asociada con un mayor riesgo de comportamientos suicidas1, por eso la importacia de un TRATAMIENTO EFECTIVO1.
La Fluvoxamina ha demostrado alivio de la depresión en pacientes con trastorno depresivo mayor y la dependencia del alcohol.2
El alivio de la depresión y la ansiedad en pacientes con dependencia del alcohol y trastorno depresivo mayor fue más rápido con fluvoxamina en comparación con otros inhibidores selectivos de recaptación de serotonina.2
Referencias
1.McHugh Rk and Weiss Rd. Alcohol Use Disorder and Depressive Disorders. Alcohol Res. 2019;40(1):arcr.v40.1.01
2. Vinnilova MA, Severtsev W, Komarov SD, et al. Fluvoxamine in the treatment of depressive disorders in alcohol dependende; results of randomized open-label comparative study. Zh Nevrol Psikhiart Im S S Korsakova. 2021:121(12):57-62.
Inicio
![]() Nota
Nota
Video Artesanos
El impacto de la música en el bienestar emocional.
Inicio
![]() Nota
Nota
TDAH EN NIÑOS
Masterclass TDAH: Resolviendo problemas en el tratamiento de NNA con trastorno por déficit de atención e hiperactividad
Inicio
![]() Nota
Nota
Luvox® tratamiento de trastorno depresivo mayor para pacientes con comorbilidades como desordenes de ansiedad y disturbio del sueño
¿Podría ser luvox® (fluvoxamina) una opción de tratamiento efectivo para sus pacientes con trastorno depresivo mayor que también tienen comorbilidades como desordenes de ansiedad y disturbio del sueño?
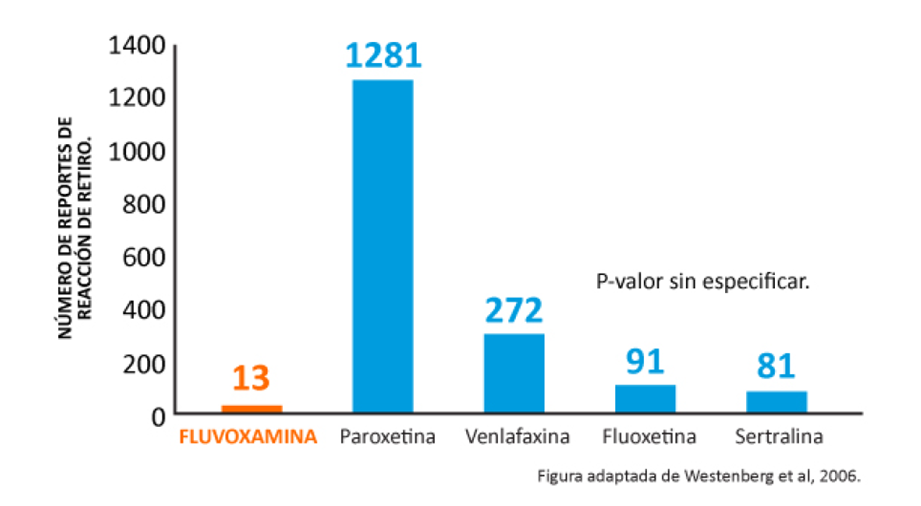
La Fluvoxamina ha exhibido menores tasas de síntomas de retiro en comparación con la paroxetina, venlafaxina, fluoxetina y sertralina en una base de datos de seguimiento del UK (2002).1
Agencia de control de medicinas uk 2002 adroit (adverse drug reactionson-line information) base de datos- de las top 20 medicinas asociadas conreportes de sospecha de reacciones de retiro.1
Referencias
1. Westenberg HGM and Sandner C. Tolerability and safety of fluvoxamine and other antidepressants. Int J ClinPract. 2006;60(4):482-491.